







The doctor examines the reproductive organs for any abnormalities.
These are used to measure hormone levels and exclude other conditions that could mimic PCOS. Additional tests might include checking glucose tolerance and cholesterol levels.
A transvaginal ultrasound is performed to check the ovaries' appearance and the uterine lining's thickness.
Periodic checks of blood pressure, glucose tolerance, and cholesterol and triglyceride levels
Screening for depression and anxiety
Screening for obstructive sleep apnea
A gynecologist must verify a pattern of symptoms in order to diagnose PMS. The symptoms must interfere with certain regular activities and be present in the five days prior to the start of a woman’s menstruation for at least three menstrual cycles. They also need to end within four days of the period beginning.



Depending on the cause, you have a wide range of therapeutic choices if your hormone levels are higher than usual. Medication, surgery, radiation therapy, or a mix of any of these are available options.
Many health conditions that involve hormonal imbalances, likely diabetes and thyroid disease, require medical treatment.

If treatment is not received, it can proceed painlessly until a bone breaks. Fractures, another name for these damaged bones, usually affect the hip, wrist, and spine.






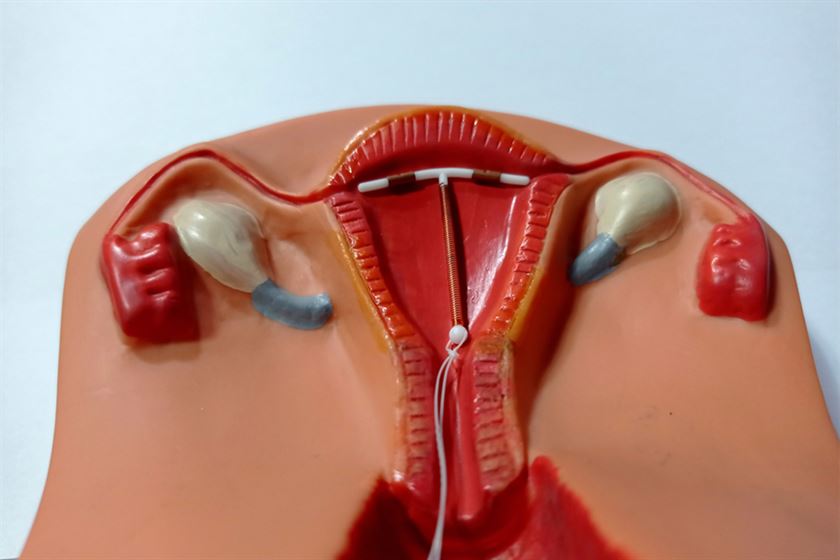
Facts about the IUD
You will learn how to feel for these threads and ensure that they are still in place from the physician who fits your IUD.
Several times throughout the first month, after every period, or on a regular basis, make sure your IUD is in place.
Although it’s unlikely that your IUD will come out, you might not be protected against pregnancy if you can’t feel the threads or believe it’s shifted.
During intercourse, your partner shouldn’t be able to feel your IUD. See a doctor or nurse for a check-up if at all possible.
